Worst Nursing Mistakes That Can Harm Patients and End Careers
A nurse walks out of a patient room and suddenly remembers that two patients with similar names were treated only minutes apart. Her heart starts racing as she mentally rechecks every patient ID and medication detail. During such moments, even experienced nurses can feel instant panic.
Across the United States, medical mistakes continue to affect hundreds of thousands of hospitalized patients every year and remain one of the leading patient safety concerns in healthcare. Some of the worst nursing mistakes happen during rushed handoffs, understaffed shifts, or emotionally exhausting nights.
Behind many nursing errors in patient safety investigations, there is often a nurse who genuinely cared but struggled with fatigue, pressure, and nonstop interruptions. This guide explains the most common medical errors nurses make, the real consequences of those mistakes, how nurses recover emotionally and professionally afterward, and the practical steps that help protect both patients and nursing licenses.
Related: What Is the Golden Rule of Bedside Care?
How One Nursing Mistake Ended Two Lives
Some stories stay with you. This is one of them. In September 2010, Kim Hiatt, a nurse with 24 years of experience at Seattle Children’s Hospital ICU, made a single dosage error. She administered a calcium chloride overdose to a fragile infant patient. The baby died. Kim was fired. Seven months later, she took her own life.
That is a fatal nursing mistake in its most devastating form. A dedicated professional, broken by guilt and isolated by consequences. Researchers later identified what Kim experienced as Second Victim Syndrome in nursing, the profound psychological trauma nurses carry after serious medical errors.
The Kim Hiatt nurse story is about what happens when good nurses work inside imperfect systems and what happens when the support they need is never there.
Discover why so many experienced critical care nurses struggle with burnout despite loving their profession.
Why Nursing Mistakes Happen: System Failure vs Individual Errors
Research continues to link nurse burnout and errors closely. According to the Agency for Healthcare Research and Quality (AHRQ), adverse events in nursing rise sharply when nurses care for more than four patients at once, yet overloaded assignments remain common in hospitals across the United States.
This table shows how failures within hospital systems and individual nurse-related factors contribute to serious nursing mistakes.
| System Failures | Individual Errors |
|---|---|
| Unsafe nurse-to-patient ratios caused by chronic understaffing. | Missing important patient details because of mental exhaustion. |
| Poor communication between departments during patient transfers. | Skipping safety double checks. |
| Increased EHR charting accuracy issues. | Documentation mistakes. |
| Lack of clear hospital protocols for high-risk situations. | Misreading medication labels or physician instructions. |
| Inconsistent shift handoff procedures between nursing teams. | Failing to communicate urgent patient updates clearly. |
None of these is in your control. All of them directly increase your risk of making a mistake.
Related: Is It Okay to Leave Bedside Nursing?
10 Worst Nursing Mistakes and Prevention Tips
Every nurse on every shift faces moments where one small decision carries enormous weight. These are the ten mistakes that show up most often in incident reports, malpractice cases, and nursing board investigations.
1. Medication Errors
Medication errors in nursing are the most common and most deadly mistakes in healthcare. Approximately 9,000 patients die annually in the U.S. from preventable medication errors.
Prevention:
- Follow the Five Rights of medication administration every single time: right patient, right drug, right dose, right route, right time.
- Use barcode scanning at the bedside before every administration.
- Always read back verbal orders to the prescribing physician before acting.
2. Charting and Documentation Errors
A nursing documentation error does not stay on paper. It travels through every hand that touches that patient next. Charting a medication you have not given yet, documenting on the wrong patient, or missing a status change creates a dangerous ripple effect across the entire care team.
Prevention:
- Chart in real time, never ahead of time, and never hours later from memory.
- Verify the patient record is open before entering any information.
- Document every clinical change, no matter how minor it seems in the moment.
3. Healthcare-Associated Infections
The Centers for Disease Control and Prevention (CDC) reports that 1 in 31 hospital patients develops a healthcare-associated infection at any given time. Many of these infections are preventable and often happen when busy staff skip hand hygiene, rush catheter care, or break sterile procedures under pressure.
Prevention:
- Follow standard precautions every single time, no exceptions for busy shifts.
- Perform proper hand hygiene before and after every patient contact.
- Maintain sterile technique even when you feel pressure to move faster.
4. Patient Falls
According to AHRQ, between 700,000 and 1 million patients fall in U.S. hospitals every year, and nearly 11,000 of those falls result in death. Nurses often contribute to patient injuries when they skip fall risk assessments, leave call lights out of reach, or leave high-risk patients unattended for even a few minutes.
Prevention:
- Complete fall risk scoring at admission and at the start of every single shift.
- Keep call lights within reach and bed alarms activated for high-risk patients.
- Round hourly on vulnerable patients. Do not wait for them to call.
5. Communication Failures
Shift changes create some of the most dangerous moments in a patient’s hospital stay. A nurse may verbally mention an important change in vital signs, but if nobody documents it correctly, that critical detail can disappear during shift change. Communication failures and SBAR breakdowns often create errors that the next nurse may never see coming until the patient’s condition suddenly worsens.
Prevention:
- Use the structured SBAR tool for every bedside report: Situation, Background, Assessment, Recommendation.
- Read back all critical lab values and new orders to confirm accuracy.
- Use a structured shift report checklist to reduce communication mistakes.
6. Missed or Delayed Assessment
Sepsis often starts with small warning signs that busy nurses can easily miss. When nurses overlook subtle changes in patients or delay escalation, patients can decline much faster than expected.
Prevention:
- Use the National Early Warning Score 2 (NEWS2) system consistently.
- Trust your clinical instincts; if something feels wrong, it probably is.
- Call the rapid response team before you are certain, not after.
7. Needlestick Injuries
This mistake may not harm the patient, but it can seriously harm the nurse. When nurses recap used needles or hasten sharps disposal, they increase their risk of exposure to HIV, Hepatitis B, and Hepatitis C.
Prevention:
- Never recap a used needle under any circumstances.
- Dispose of sharps immediately into an approved container at the point of care.
- Always report every needlestick to occupational health within the hour.
8. Disregarding Safety Protocols
Ignoring patient ID checks, hurrying surgical timeouts, or bypassing medication alerts may seem harmless during a stressful shift, but these shortcuts can lead to dangerous mistakes. Hospitals create safety rules because previous errors harmed real patients.
Prevention:
- Take the 30 seconds that a safety protocol requires.
- Never overrule a medication alert without documenting a clinical reason.
- Treat every patient identifier check as non-negotiable, regardless of how well you know the patient.
9. Ignoring Nurse Fatigue
Nurses working beyond 12 hours are three times more likely to make an error. Fatigue is not a personal weakness. It is a clinical risk factor.
Prevention:
- Recognize the signs of dangerous fatigue in yourself before they affect your patients.
- Use buddy checks at the end of long shifts.
- Advocate for safe scheduling. Your stress is a patient safety issue, not just a personal one.
10. Not Speaking Up for the Patient
A nurse silenced by physician hierarchy. A gut feeling ignored. A rapid response call was delayed because of fear. Patients deteriorate in the gap between what a nurse knows and what she feels safe saying out loud.
Prevention:
- Using SBAR gives your concern a clinical structure that is hard to dismiss.
- Follow your hospital’s chain of command if a physician dismisses a legitimate safety concern.
- Document every concern you raise and every response you receive in real time.
Related: Toxic Hospital Culture for Nurses
Common New Nurse Mistakes That Affect Patient Safety
Your first year of nursing will teach you more than any classroom ever could. It will also expose you to a specific set of nursing errors in the first year because nursing school prepares you for the theory, and the floor prepares you for the reality. These are the new nurse mistakes that first-year veterans wish someone had warned them about earlier.
- Charting in advance means documenting care before giving it.
- Rushing medication checks without completing all five safety steps.
- Not asking for help, because they fear embarrassment.
- Forgetting to remove an old transdermal patch before applying a new one.
- Discharging a patient while an IV saline lock remains in place.
Pro Tip: Nurses who speak up and double check details usually grow faster and make safer decisions.
Related: How Can Nurse Managers Improve Nurse Morale?
What Happens After a Nursing Mistake: License, Legal, and Career Consequences
Most nurses who make a mistake spend the first hours after it asking the same terrifying question: how bad does this get? The honest answer depends entirely on what the mistake was, how it happened, and what you did next.
State Nursing Board Disciplinary Actions
This video explains how one nursing medication error led to criminal charges, probation, license consequences, and a nationwide debate about error reporting in healthcare.
Nursing license discipline follows a structured progression. Understanding each level helps you see that most single honest mistakes do not end careers. The question of whether a nurse can lose their license for a mistake has a real answer: rarely, if it was a genuine, isolated error handled with transparency.
Below are the most common nursing board disciplinary actions:
▴ Informal reprimand: The nursing board issues a private warning for minor mistakes or first-time low-risk errors. Nurses usually keep working without major license restrictions.
▴ Formal censure: The board places an official disciplinary warning on the nurse’s public record. This often happens after repeated ongoing concerns.
▴ Probation with conditions: The nurse may continue working under supervision, education requirements, or practice restrictions. Boards commonly use probation after medication or patient safety errors.
▴ Suspension: The board temporarily removes the nurse’s license because of repeated unsafe behavior. Nurses cannot legally practice during the suspension period.
▴ Revocation: The board permanently removes the nursing license after extreme negligence, criminal conduct, or intentional patient harm. This is the most serious disciplinary action possible.
Safety Tip: If a mistake happens, immediately document your patient load, staffing shortages, equipment problems, and communication issues. Those details may help protect your nursing license and professional record later.
Related: Nurses Crying After Work
How Should Nurses Report a Nursing Error?
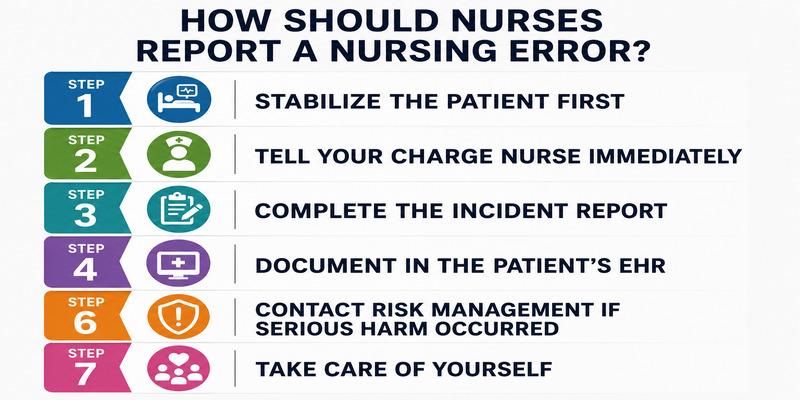
Reporting a mistake feels terrifying. But the steps you take in the next hour matter more than the mistake itself. Here is exactly what to do.
Step 1: Stabilize the patient first. Address any immediate harm before anything else. Your patient comes before the paperwork always.
Step 2: Tell your charge nurse immediately. Do not wait, do not overthink it. Your charge nurse needs to know right now.
Step 3: Complete the incident report accurately and promptly. The incident report nursing process exists to protect you and improve the system.
Step 4: Document in the patient’s EHR. Record what happened, what intervention you provided, and how the patient responded. Be factual and document in real time.
Step 6: Contact risk management if serious harm occurred. If the error caused significant patient harm, your risk management team needs to be in the loop before anyone else asks questions.
Step 7: Take care of yourself. Reach out to peer support or your hospital’s Employee Assistance Program. What you are feeling right now is real, and you deserve support too.
Related: How to Survive Night Shift as a Nurse
How Do Nurses Recover After a Mistake
Making a mistake as a nurse does not just affect your patient. It follows you home. It sits with you at dinner. It wakes you up at 3 AM, replaying every decision you made that shift. The emotional impact of nursing mistakes is real.
What Is Second Victim Syndrome?
Second victim syndrome in nursing was first defined by Dr. Albert Wu of Johns Hopkins University to describe what happens to healthcare providers after they are involved in a serious medical error. The term exists because the experience needed a name.
Research shows that two-thirds of providers involved in medical errors report:
- Extreme sadness that does not lift after a few days.
- Difficulty concentrating during subsequent shifts.
- Clinical depression requires professional support.
- A persistent sense of guilt that ordinary self-care does not resolve.
This is a documented psychological response to trauma, and it happens to skilled, experienced, deeply committed nurses every single day.
For deeper context, study the 42% rule for burnout to understand how emotional exhaustion can affect decision making during long nursing shifts.
Signs of Second Victim Syndrome in Nurses
Watch for these signs in yourself:
- Intrusive thoughts about the incident that replay during or after your shift.
- Avoidance of similar patient situations, specific procedures, or the unit where the error occurred.
- Difficulty returning to normal clinical function even after time has passed.
- Isolation from colleagues because you feel too ashamed to talk about what happened.
- Depression or suicidal ideation that develops in the weeks following the incident.
If you recognize yourself in this list, please take it seriously. They are a sign that you need real support right now.
Feeling mentally exhausted? Try this quick nurse burnout and stress level checker tool to better understand your current stress load.
Where to Get Support: Peer Hotlines and Programs
You do not have to carry the syndrome experience alone. These programs exist specifically for healthcare providers in your situation:
- RISE Program at Johns Hopkins: Resilience In Stressful Events, a peer support model designed specifically for second victims of medical errors
- University of Missouri 24/7 Peer Support Line: Staffed by trained healthcare peers who understand exactly what you are going through
- Hospital Employee Assistance Programs (EAP): Confidential mental health support available through your employer at no cost.
- American Nurses Association Mental Health Resources: Available at nursingworld.org for nurses seeking professional guidance
If you are experiencing suicidal thoughts right now, please call or text 988 to reach the Suicide and Crisis Lifeline. It is available 24 hours a day, seven days a week.
Related: How Nurses Can Exercise with a Busy Work Schedule
Frequently Asked Questions
Can AI charting systems increase nursing mistakes?
Yes. Many hospitals now use AI-assisted charting and predictive healthcare software, but these systems can still create documentation errors if nurses rely too heavily on automation. Incorrect autofill information, copied notes, or missed alerts may increase patient safety risks. Nurses still need to verify every chart entry carefully. I always recommend double-checking important patient information instead of trusting automated systems completely.
Can nurses face discipline for using ChatGPT or AI tools at work?
Yes. Some hospitals restrict nurses from using AI tools to document patient information, summarize charts, or assist with clinical decisions. Sharing protected patient data with unauthorized AI platforms may create HIPAA and patient privacy risks. Many healthcare systems now develop AI policies specifically for nurses and clinicians to prevent unsafe practices.
Are virtual nurses changing bedside patient safety?
Many hospitals now use virtual nurses through video monitoring systems to assist with charting, discharge education, and patient observation. Supporters believe virtual nursing helps reduce burnout and staffing pressure, while critics worry technology may weaken direct bedside assessment and communication. Hospitals continue studying whether virtual care improves patient safety or increases the risk of the worst nursing mistakes caused by missed in person observations. I believe technology works best when it supports bedside nurses instead of replacing direct patient care.
Also read: Can You Die from Overworking?
Conclusion
Learning about the worst nursing mistakes is not about creating fear or blame. It is about building safer habits, stronger communication, and healthier support systems for both nurses and patients.
If you work in healthcare, give yourself permission to slow down, ask questions, and speak up when something feels wrong. Small safety steps often prevent the biggest problems later. Most importantly, remember that one difficult moment does not define your entire career. Nurses carry an incredible amount of responsibility every day, and they deserve support just as much as the patients they care for.
Also read: Caregiver Burnout vs Compassion Fatigue
Refrences
- https://en.wikipedia.org/wiki/RaDonda_Vaught_homicide_case
- https://www.cdc.gov/healthcare-associated-infections
- https://www.ncbi.nlm.nih.gov/books/NBK519065
- https://www.ahrq.gov/topics/falls.html
Disclaimer: This content is for educational purposes only and should not replace professional medical, legal, or mental health advice.