10 Tested Tips for Preventing Healthcare Staff Burnout: A 2026 Evidence-Based Guide for Nurses and Hospital Leaders
Behind every staffing shortage stands a healthcare worker who covers another shift, loses valuable recovery time, and carries the emotional strain home. Emotional stress remains a major reason nurses leave their roles.
The pressure extends across the healthcare system, where 1.1 million physicians serve 340 million Americans, and new patients wait an average of 26 days for an appointment. The American Hospital Association also projects that the United States could have 64,000 fewer nurses by 2030. Healthcare organizations can no longer treat burnout as a personal weakness or a temporary concern.
I will share 10 tested tips for preventing healthcare staff burnout that can improve workloads, leadership, and workplace culture.
This guide supports two groups: nurses and frontline healthcare workers who need practical help now, and nurse managers, hospital administrators, and HR leaders who can drive organizational change. Both perspectives matter.
What Is Healthcare Staff Burnout?
Healthcare burnout refers to a work-related pattern of emotional exhaustion, interpersonal detachment, and reduced professional confidence that develops under prolonged occupational pressure.
Stress can be short-term or ongoing, while burnout develops from persistent workplace stress and often involves exhaustion, cynicism, and reduced motivation. Burnout can affect anyone in healthcare, including nurses, physicians, technicians, therapists, aides, administrative staff, and support workers.
Burnout is not a character flaw, a lack of dedication, or proof that someone chose the wrong career. It often reflects an unhealthy gap between job demands and available support.
Burnout can feel permanent when exhaustion continues for months, but recovery is possible. Learn more about whether burnout is permanent and what the recovery process may look like.
Not sure how much pressure you are carrying? Use our stress level checker tool for a quick self-assessment and a clearer view of your current stress patterns.
Burnout vs. Compassion Fatigue vs. Moral Injury: Key Differences
Healthcare workers may experience these forms of occupational distress simultaneously, but each has a distinct primary trigger.
| Experience | Core Features | Common Drivers |
|---|---|---|
| Burnout | Low energy, emotional withdrawal, and reduced professional effectiveness. | Heavy workloads, limited control, administrative pressure, and organizational problems. |
| Compassion Fatigue | Emotional depletion, reduced empathy, and distress are linked to caring for suffering patients. | Repeated exposure to illness, trauma, grief, and emotional pain. |
| Moral Injury | Guilt, shame, anger, betrayal, or helplessness after a perceived violation of professional values. | Being unable to provide the standard of care a clinician believes a patient needs. |
For example, an ICU nurse may experience moral distress when an unsafe workload prevents timely patient care. If that experience leads to lasting guilt, anger, or a sense of betrayal, it may contribute to moral injury.
The Stages of Burnout in Healthcare Workers
Psychologists Herbert Freudenberger and Gail North proposed a 12-phase model that describes patterns sometimes associated with worsening burnout:
The 12 Stages of Burnout
- Excessive drive or ambition, often described as the “hero” phase.
- Pushing yourself harder to meet impossible demands.
- Neglecting personal needs, including sleep, nutrition, and social connection.
- Displacing conflict by blaming patients, colleagues, or the system.
- Revising personal values until work becomes the main priority.
- Denying emerging problems.
- Withdrawing from social life and outside interests.
- Showing noticeable behavioral changes, such as irritability or emotional withdrawal.
- Experiencing depersonalization, such as identifying patients only by their condition or room number.
- Experiencing emptiness or loss of meaning.
- Developing symptoms that may overlap with depression.
- Reaching severe occupational burnout.
These phases do not form a fixed clinical timeline, and a person may experience them in a different order or skip some entirely. Recognizing changes in energy, behavior, and connection to work can help healthcare workers identify growing concerns before they intensify.
What Causes Healthcare Worker Burnout?
To prevent burnout effectively, healthcare organizations must first understand the conditions that place employees under sustained pressure.
Below, we explore the key factors that contribute to burnout among healthcare workers.
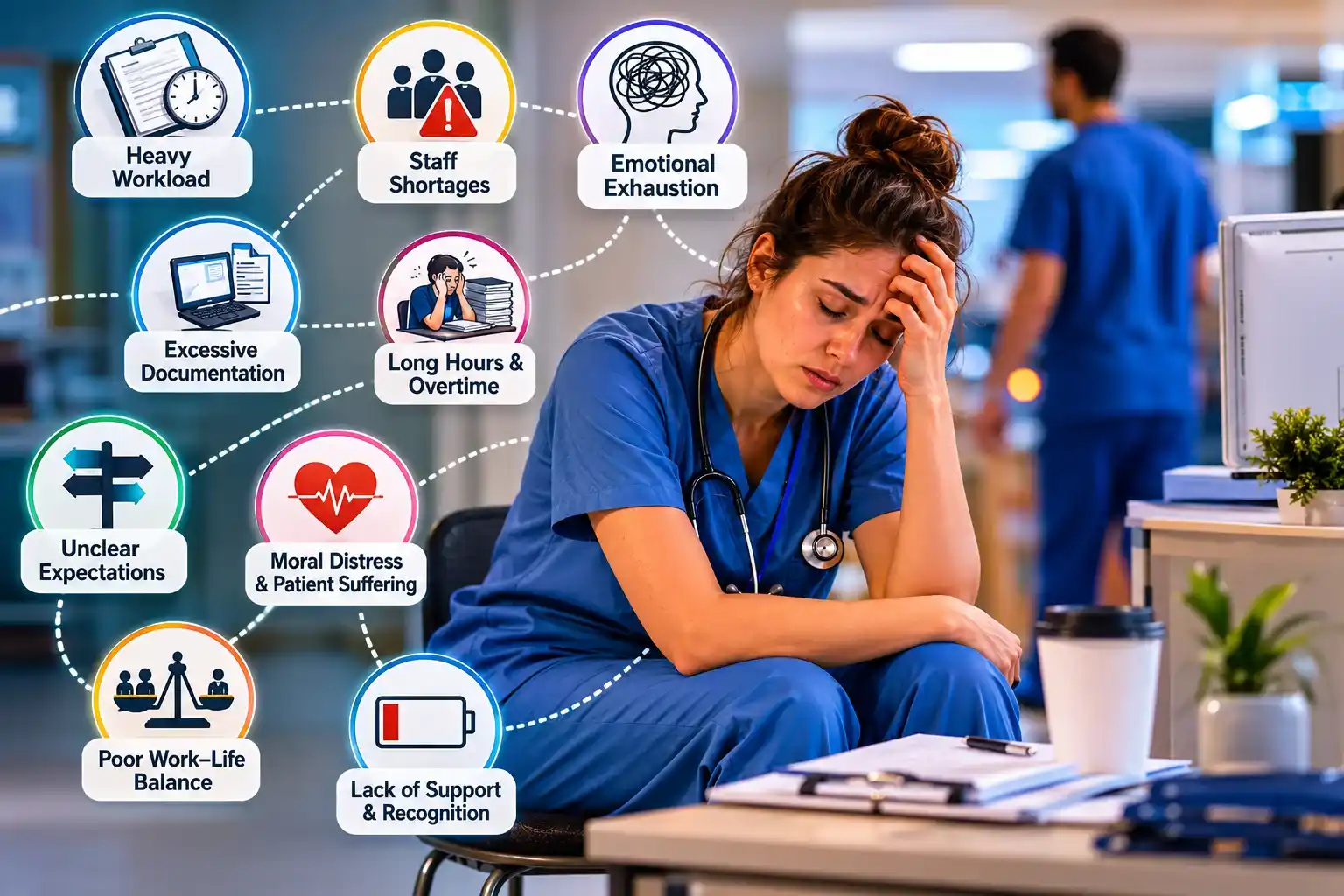
System-Level Pressures
- Chronic understaffing and heavy patient assignments.
- Long shifts, frequent overtime, and limited recovery time.
- Excessive documentation, EHR demands, and nonclinical tasks.
- Inefficient workflows and frequent interruptions.
- Rising patient complexity and increasing demand for care.
Workplace and Leadership Problems
- Unsupportive or controlling management.
- Limited employee input in scheduling and clinical decisions.
- Unclear expectations and poor communication.
- Bullying, hostility, or unhealthy team dynamics.
- Inadequate recognition and limited career growth.
- Discrimination, unfair treatment, or low psychological safety.
- Poor coordination across teams and departments.
Emotional and Ethical Demands
- Repeated exposure to illness, trauma, suffering, and death.
- Moral distress when limited resources prevent staff from providing the care they believe patients need.
- Workplace violence, threats, or harassment.
- Pressure to make high-stakes decisions under difficult conditions.
- Emotional strain from supporting distressed patients and families.
Personal and Contextual Risk Factors
- Perfectionism and difficulty asking for support.
- Poor boundaries between work and personal life.
- Limited social support outside the workplace.
- Financial pressure, student debt, or job insecurity.
- Sleep disruption from night shifts or rotating schedules.
- Limited access to healthy coping strategies or recovery time.
10 Tested Tips for Preventing Healthcare Staff Burnout
This is where the rubber meets the road. Each tip below is grounded in published research and documented hospital programs. I have structured each one to address both what administrators can do systemically and what nurses can do personally within that same domain.
Tip 1: Address Staffing Ratios and Workload at the Institutional Level
This one is non-negotiable. Meditation apps and resilience training cannot offset the strain of unsafe patient assignments.
What hospital leaders can do:
- Review staffing levels every quarter using patient acuity, not census numbers alone.
- Support state policies that establish safe nurse-to-patient staffing standards.
- Use float pools and cross-training to cover staffing gaps without overloading other employees.
- Use predictive staffing models (now available through several EHR platforms) to anticipate high-census periods
What nurses can do:
- Report unsafe assignments through your hospital or union’s approved process, using an ADO form or equivalent when available.
- Contact your union, state nursing association, or National Nurses United for staffing and advocacy resources.
- Review your facility policies, union agreement, state laws, and applicable OSHA protections before taking action.
Use the American Nurses Association’s current safe-staffing resources to guide conversations about workloads and staffing practices.
Tip 2: Implement and Actively Promote Employee Assistance Programs (EAPs)
Employee Assistance Programs are available in many hospital systems, but some healthcare workers hesitate to use them because of stigma, limited awareness, or concerns about confidentiality. Clear communication about privacy, eligibility, and available services can help build trust.
What hospital leaders can do:
- Actively communicate that EAP use is confidential and cannot affect employment or licensure.
- Bring EAP counselors on-site during high-stress periods (after mass casualty events, COVID surges, or high-profile patient deaths).
- Expand EAP services to include financial counseling, childcare referrals, and legal assistance, which address the full picture of nurse stress.
- Partner with Healthy Nurse, Healthy Nation, a free ANA Enterprise wellness program that offers resources for nurses and healthcare organizations.
What nurses can do:
- Contact your EAP to confirm counseling, costs, confidentiality rules, and any limits that apply to your plan.
- Ask whether your EAP offers financial counseling or referrals for concerns such as student debt or rising living costs.
- If you are in emotional distress or a suicidal crisis in the United States, call or text 988 for free, confidential support. Call 911 if you or someone else faces immediate danger.
Tip 3: Reduce EHR Administrative Burden Through Technology and Policy
EHR burnout is real, documented, and increasingly addressable through both technology and policy intervention. The Joint Commission has published standards on workforce well-being that include documentation burden as a systemic issue hospitals must address.
What hospital leaders can do:
- Review how staff spends documentation time, identify the most burdensome tasks, and remove unnecessary duplication.
- Invest in AI-assisted documentation tools that may reduce documentation time while maintaining clinician review, patient privacy, and organizational oversight.
- Implement scribes or documentation support staff for high-volume settings.
- Create a Documentation Burden Reduction Committee that includes bedside nurses, not just administrators and informatics specialists.
What nurses can do:
- Use every available efficiency tool in your EHR system.
- Submit formal feedback through your hospital’s shared governance structure when documentation workflows are unnecessarily burdensome.
- Connect with nurse informaticists in your organization. They are your allies in fighting bad system design
Tip 4: Create Psychologically Safe Work Environments
Psychological safety means employees feel able to ask questions, raise concerns, or acknowledge mistakes without fear of embarrassment or retaliation. Amy Edmondson’s research links psychological safety in healthcare with open communication, stronger teamwork, employee well-being, and patient safety.
In hospitals where psychological safety is low, nurses do not report near-misses, do not ask for help when overwhelmed, and do not disclose burnout symptoms until they are in crisis.
What hospital leaders can do:
- Train charge nurses and nurse managers in psychologically safe leadership behaviors (asking for input, responding non-defensively to concerns, following up on reported issues).
- Implement anonymous reporting systems for culture and safety concerns that are visibly acted upon.
- Address lateral violence and bullying with zero tolerance and transparent disciplinary action.
- Conduct regular pulse surveys and share the results with staff, including what will change.
What nurses can do:
- Recognize that speaking up about unsafe conditions is a professional and ethical obligation under the ANA Code of Ethics.
- Practice the CUS tool (Concerned, Uncomfortable, Safety issue) for assertive communication in high-stress moments.
- Build trusted relationships with one or two colleagues you can debrief with after difficult shifts.
Tip 5: Establish Peer Support Programs and Mentorship Networks
After critical incidents, nurses are frequently told to “debrief” in a rushed, mandatory group session before going home. This approach is largely ineffective and can retraumatize. Structured peer support programs, designed and led by trained peers rather than administrators, have significantly better outcomes.
What hospital leaders can do:
- Consider a structured peer-support program such as Resilience in Stressful Events (RISE), developed at Johns Hopkins Hospital, which trains healthcare workers to support colleagues after stressful work-related events.
- The RISE model has been replicated across dozens of health systems and has documented outcomes: nurses who access peer support after a critical event return to work faster, report lower distress, and are less likely to leave.
- Create formal mentorship programs that pair experienced nurses with new graduates for the first two years of practice, when nurse burnout risk is highest.
- Support the development of specialty-specific peer networks (ICU nurses supporting ICU nurses; oncology nurses supporting oncology nurses).
What nurses can do:
- Seek out a mentor, formally or informally. Nurses who report having a professional mentor show significantly higher job satisfaction and lower burnout rates.
- Offer to be a peer supporter. Helping others process difficult experiences is itself protective against burnout.
- Connect with nursing communities on professional platforms and specialty organizations such as the American Association of Critical-Care Nurses (AACN).
Tip 6: Protect Rest, Breaks, and Work-Life Boundaries Institutionally
This tip sounds obvious. It is not obvious to many hospital systems that routinely schedule nurses for three consecutive 12-hour night shifts, deny lunch breaks, and call staff in on scheduled days off.
What hospital leaders can do:
- Schedule protected meal and rest breaks with adequate relief coverage, while following applicable state laws, workplace policies, and collective bargaining agreements.
- Eliminate mandatory overtime wherever possible. Nurses who work more than 12 consecutive hours are significantly more likely to make medication errors, according to AHRQ research.
- Schedule a minimum of 12 hours between shifts and 48 hours off per week.
- Create quiet rest spaces on units where nurses can decompress between patients.
- Implement scheduling software that distributes weekend, holiday, and night-shift burden equitably.
What nurses can do:
- Take your breaks. I know this sounds simplistic, but nurses are trained to put others first, and break-skipping becomes habitual. Your break is not selfish. It makes you safer
- Set communication boundaries outside of work hours. If your manager expects text responses on your days off, that expectation needs a direct, calm conversation.
- Prioritize sleep hygiene aggressively, especially for night shift nurses. The ANA’s Healthy Nurse, Healthy Nation program offers free sleep resources.
Tip 7: Build Career Development and Recognition Programs
Nurses who feel professionally stagnant and unrecognized leave. Is it that straightforward? Recognition is not the same as a pizza party. It is a visible acknowledgment of clinical expertise and a clear pathway forward.
What hospital leaders can do:
- Implement a clinical ladder program that rewards bedside expertise with both financial compensation and title advancement.
- Create structured opportunities for nurses to present at grand rounds, contribute to research, or lead quality improvement projects.
- Build transparent promotion pathways that do not require nurses to move into administration to advance their careers.
- Recognize nurses by name and specific action in public forums, not just anonymously in a “staff of the month” poster.
- Offer tuition reimbursement or education support for advanced nursing degrees and professional certifications.
What nurses can do:
- Pursue specialty certification in your practice area. Certified nurses report higher job satisfaction, higher perceived competence, and lower burnout rates than non-certified peers, according to AHRQ data.
- Join your hospital’s shared governance councils. Nurses with a voice in institutional decisions experience significantly lower burnout.
- Document your impact. Keep a professional portfolio of patient outcomes, quality metrics, and projects you have led. This is the evidence base for your own advancement.
Tip 8: Support Recovery Through Regular Physical Activity
Regular exercise can support mood, sleep, energy, and stress management. Choose activities that fit your health, schedule, and fitness level. Even with a busy work schedule, short and realistic exercise sessions can support consistency.
- Take a brisk walk before or after a shift.
- Practice gentle yoga to improve flexibility and relaxation.
- Cycle outdoors or use a stationary bike.
- Complete short strength-training sessions at home or in the gym.
- Use stretching or mobility exercises during breaks.
- Try swimming, dancing, or another activity you enjoy.
- Start with short sessions and increase gradually.
- Choose consistency over intense or unrealistic routines.
Stop exercising and seek medical advice if you experience chest pain, severe shortness of breath, dizziness, or unusual symptoms.
Tip 9: Plan Balanced Meals Around Your Health Needs
Long shifts and unpredictable schedules can make healthy eating difficult for healthcare workers. Planning simple, balanced meals can support steady energy and reduce the temptation to skip meals during busy shifts.
- Build balanced meals with protein, whole grains, fruits, vegetables, and healthy fats.
- Prepare portable meals and snacks for long or unpredictable shifts.
- Use a calorie deficit only when weight loss is an appropriate personal goal. Choose a gradual, realistic approach instead of severe restriction. Use our calorie calculator to estimate your daily calorie needs and plan meals around your health goals.
- Consider intermittent fasting only if it works with your shifts, health needs, and medications. It is optional, not a burnout treatment.
- Avoid calorie restriction or fasting if you have an eating disorder or a history of disordered eating unless a qualified healthcare professional guides you.
- Seek advice from a physician or registered dietitian if meal timing, weight goals, or health conditions make planning difficult.
Tip 10: Make Time for Hobbies That Restore Your Energy
Hobbies can help healthcare workers mentally disconnect from work and reconnect with life outside the hospital.
- Read a book, journal, or listen to music.
- Try gardening, painting, photography, or crafts.
- Cook or bake something you enjoy.
- Spend time outdoors or in nature.
- Play an instrument or learn a creative skill.
- Start with 10 to 20 minutes on busy days.
- Choose activities that feel relaxing, not demanding.
- Avoid turning hobbies into another performance goal.
- Focus on enjoyment, recovery, and emotional balance.
To learn how sleep, exercise, meals, and downtime can support recovery, read our guide to the 42% rule for burnout.
Sample Scripts for Workload and Schedule Concerns
Use clear, professional language and focus on workload, scheduling, and available support.
To raise workload concerns:
“I am finding the current workload difficult to manage safely. Can we discuss staffing, task priorities, or other support options?”
To request a schedule change:
“My current schedule is affecting my ability to recover between shifts. I want to discuss a temporary adjustment or other available options.”
To follow up:
“Thank you for discussing this with me. Can we agree on the next steps and a date to review whether the changes are helping?”
Real Hospital Programs Supporting Healthcare Worker Well-Being
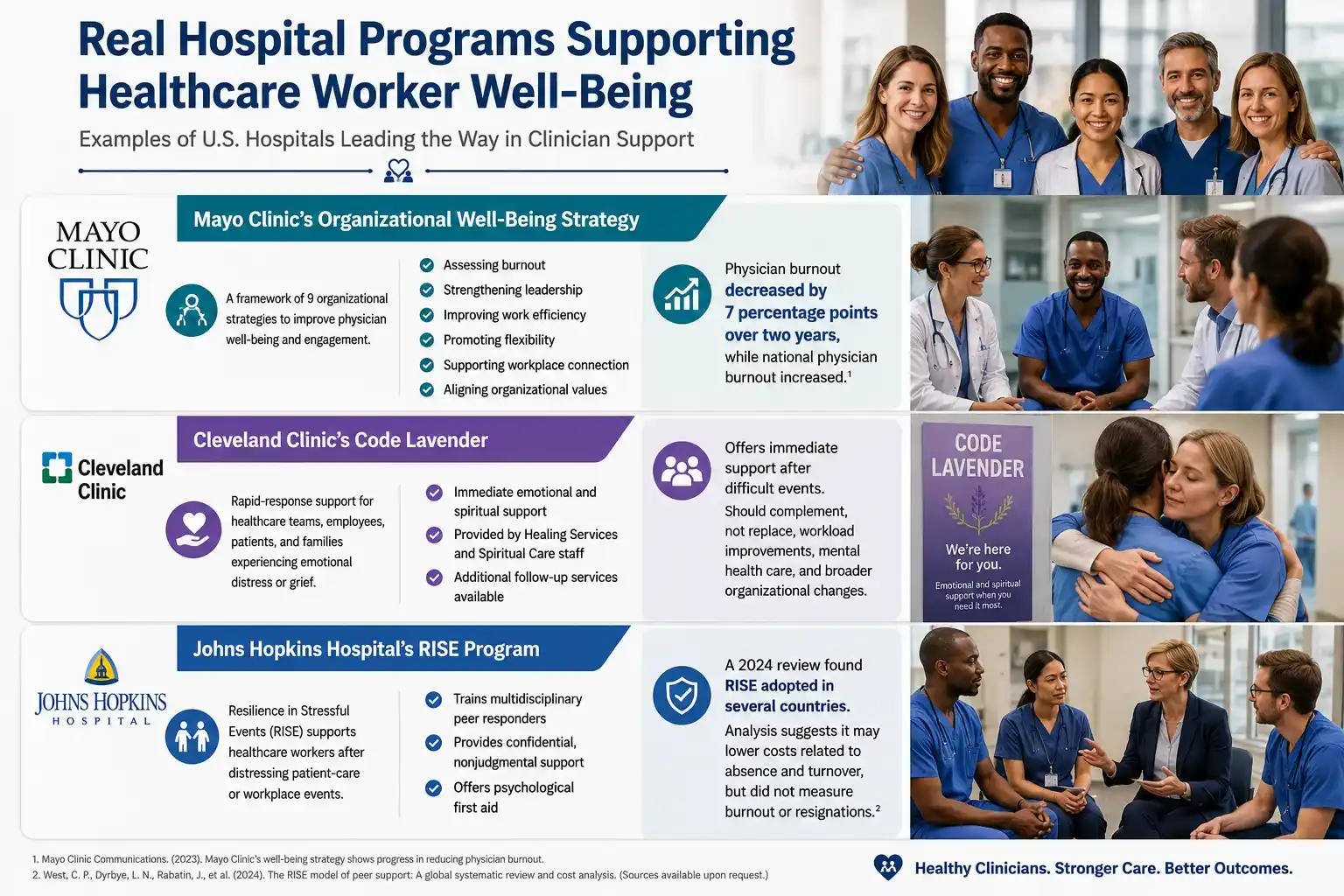
Some U.S. hospitals have introduced structured programs to support healthcare workers after stressful events and improve workplace well-being. The examples below show how different organizations approach clinician support.
Mayo Clinic’s Organizational Well-Being Strategy
Mayo Clinic leaders published a framework of nine organizational strategies designed to improve physician well-being and engagement. The approach included assessing burnout, strengthening leadership, improving work efficiency, promoting flexibility, supporting workplace connection, and aligning organizational values.
Mayo Clinic reported that physician burnout decreased by seven percentage points over two years, while national physician burnout increased. Because the organization introduced several changes during that time, the result should not be attributed to a single intervention alone.
Cleveland Clinic’s Code Lavender
Cleveland Clinic uses Code Lavender as a rapid-response support service for healthcare teams, employees, patients, and families experiencing emotional distress or grief. Healing Services and Spiritual Care staff provide personalized emotional and spiritual support, with additional services available after the initial response.
Code Lavender offers immediate support following difficult events, but it should complement, rather than replace, workload improvements, professional mental health care, and broader organizational changes.
Johns Hopkins Hospital’s RISE Program
Johns Hopkins Hospital established the Resilience in Stressful Events program, known as RISE, to support healthcare workers after distressing patient-care or workplace events. The program trains multidisciplinary peer responders to offer confidential, nonjudgmental emotional support and psychological first aid.
A 2024 review found that healthcare organizations in several countries had adopted the RISE model. A separate analysis suggested that the program may lower costs linked to staff absence and turnover, but it did not directly measure burnout or resignation rates.
Frequently Asked Questions About Healthcare Burnout
What is the Maslach Burnout Inventory?
The Maslach Burnout Inventory (MBI) is one of the most widely used research tools for assessing burnout in healthcare and other professions. Christina Maslach and Susan E. Jackson first published the instrument in 1981. The healthcare version measures emotional exhaustion, depersonalization, and personal accomplishment. The MBI is available through Mind Garden for licensed individual, organizational, and research use. It measures burnout patterns along a continuum, but it does not provide a clinical diagnosis.
How long does it take to recover from nurse burnout?
Recovery from nurse burnout varies significantly based on severity, access to support, and whether the underlying systemic causes are addressed. Mild to moderate burnout, caught early and treated with a combination of reduced workload, counseling, and behavioral change, can show meaningful improvement in 3 to 6 months. Severe burnout or burnout complicated by depression, PTSD, or substance use typically requires longer, structured professional treatment. Recovery is not linear, and returning to the same environment that caused burnout without systemic change is unlikely to produce lasting recovery.
Should I leave healthcare, change departments, or reduce my hours because of burnout?
There is no single right choice. Start by identifying whether burnout comes mainly from your current department, schedule, workload, manager, or the healthcare field itself. A temporary reduction in hours, schedule change, leave of absence, or transfer to another unit may help you evaluate your options without making an immediate career exit.
How can healthcare workers recover when they cannot take extended time off?
Healthcare workers who cannot take extended time off should focus on reducing the strain that continues between shifts. This may include limiting extra shifts, protecting meal and rest breaks, improving sleep consistency, and asking for temporary schedule or workload adjustments. Short recovery periods can help, but they will not fully resolve burnout if understaffing, excessive demands, or poor workplace support continue. Lasting recovery usually requires both personal rest and changes to the conditions causing the burnout.
Why do some hospital burnout programs fail?
Programs often fail when organizations offer wellness apps, resilience training, or appreciation events without addressing workloads, staffing gaps, poor leadership, or administrative burden. Employees may also lose trust when leaders collect feedback but do not communicate or act on the results.
Bottom line
Healthcare worker burnout is not always a failure of personal resilience. When workplace systems repeatedly prevent clinicians from providing the care they believe patients need, the deeper problem may be moral injury. In such cases, real improvement requires organizational change, not simply more self-care.
Disclaimer: This article was reviewed for clinical accuracy. Always consult your healthcare institution’s Employee Assistance Program or a licensed mental health professional for personalized support.
References
- National Academy of Medicine. (2021). Clinician Well-Being Knowledge Hub.
- Agency for Healthcare Research and Quality (AHRQ). (2022).
- Maslach Burnout Inventory Manual (3rd ed.)
- Preventing a parallel pandemic: a national strategy to protect clinicians’ well-being.
- 988 Suicide and Crisis Lifeline.
- The Emotional PPE Project.
- 2026 NSI National Health Care Retention & RN Staffing Report