Back Pain in Healthcare Workers: Causes, Risks, and Prevention Tips
Quick Answer: Back pain is one of the most common work-related musculoskeletal problems in healthcare. NCBI StatPearls reports that nurses and operating room staff have annual back-pain rates of 40–50% and lifetime rates of about 80%.
Back pain in healthcare work is rarely caused by a single shift. Patient transfers, long hours on your feet, repeated bending, awkward posture, and physical fatigue can all place stress on the spine.
Back pain in healthcare workers may start as mild soreness, but the pattern matters. Pain that improves with rest may point to routine strain, while pain that worsens, spreads, causes weakness, or keeps returning may need medical evaluation.
This article is for nurses, RNs, CNAs, LPNs, OR technicians, and other healthcare workers who want to understand why their back hurts, recognize key warning signs, and reduce strain through safer daily work habits.
The Back Pain Crisis in Healthcare: Key Statistics
Recent BLS data show that health care and social assistance remains a high-injury sector, with an injury and illness rate of 3.4 cases per 100 full-time workers. For back-related risk, CDC/NIOSH identifies patient handling, including manual lifting, moving, and repositioning patients, as the single greatest work-related musculoskeletal disorder risk factor for healthcare workers.
OSHA estimates that direct and indirect costs associated with back injuries in the U.S. healthcare industry reach about $20 billion annually. These costs include the wider impact of injuries, lost productivity, and workplace disruption. Beyond the financial burden, back pain can affect healthcare workers’ mobility, job performance, and long-term ability to stay in patient care roles.
Back Pain in Healthcare Workers: Common Causes and Risk Factors
Work-related back pain often builds gradually and can affect comfort, focus, and job performance. Before looking at specific risk factors, it helps to understand why healthcare settings place unique physical demands on the body.
The primary drivers are:
- Patient handling: manual lifting, moving, transferring, or repositioning patients. CDC/NIOSH identifies patient handling as one of the most important work-related musculoskeletal risks for healthcare workers.
- Repeated bending and twisting: tasks like changing beds, assisting with hygiene, reaching across beds, or working around equipment can place repeated stress on the lower back.
- Long hours of standing and walking: long shifts can fatigue the back, hips, and legs, making posture and movement harder to control.
- Awkward postures: leaning over patients, working in tight spaces, or holding the body in uncomfortable positions can increase spinal strain.
- Overexertion and poor body mechanics: sudden movements, lifting without help, or using the back instead of legs and core can contribute to strain.
- Fatigue, poor sleep, and high workload: StatPearls notes that physical demands, long working hours, patient handling, and demanding schedules are major contributing factors for low back pain in healthcare professionals.
- Psychosocial stress: high job demands, low support, burnout, and stress can also contribute to low back pain risk and recovery problems.
Additional risk factors include:
- Night shift compounds fatigue and reduces the available staff for assisting with lifts.
- High patient-to-nurse ratios can limit time for proper equipment use.
- Inadequate staffing for two-person transfers.
- Old or unavailable mechanical lift equipment.
- Slippery floors and cluttered patient room layouts.
- Pre-existing musculoskeletal vulnerabilities aggravated by repeated strain.
Want to understand your current stress level? Try our free Stress Level Checker tool to get a quick self-check and better understand how stress may be affecting your wellbeing.
High-Risk Patient Handling Tasks for the Spine

Some patient-care tasks place more strain on the back than others, especially when they involve heavy lifting, awkward posture, sudden movement, pushing or pulling force, or working without enough support.
| High-Risk Task | Why It Can Strain the Spine | Safer Option to Consider |
|---|---|---|
| Lifting a patient from the floor. | High spinal load and awkward body position. | Mechanical full-body lift with trained assistance. |
| Repositioning a patient in bed manually. | Repeated pulling and forward bending. | Slide sheet, repositioning sheet, or ceiling lift. |
| Bed-to-chair pivot transfer without support. | Sudden weight shift and twisting. | Gait belt, sit-to-stand lift, or trained two-person assist. |
| Boosting a patient up in bed. | Forward bending under load. | Repositioning the sheet with lift assistance. |
| Assisting ambulation without a gait belt. | Sudden load if the patient stumbles. | Transfer belt and appropriate staff support. |
| Holding a limb during procedures. | Static load and awkward posture. | Positioning aids, limb supports, or team assistance. |
The key takeaway is simple: safer patient handling depends on using the right equipment, enough trained help, and facility-approved procedures before the task becomes an injury risk.
Back Pain Risk by Healthcare Role
Back strain does not affect every healthcare worker in the same way. Each role creates its own physical challenges during daily patient care.
Back pain prevention should align with the worker’s role, work setting, and daily tasks. A bedside nurse, home health aide, OR technician, and EMT may all face back strain, but the safest solution depends on the work environment and available support.
How Chronic Back Pain Can Affect a Healthcare Career
Chronic back pain can affect more than physical comfort. For healthcare workers, ongoing pain may affect daily work in several ways:
- Reduced mobility: Routine movements may feel harder or more limited during a shift.
- Lower focus during patient care: Pain can make it difficult to concentrate during high-pressure tasks.
- Fear of reinjury: Workers may feel anxious before physically demanding assignments.
- Sleep disruption: Post-shift discomfort may disturb sleep and reduce recovery, especially for night-shift or rotating-shift workers.
- More fatigue: Poor recovery can make the next shift feel harder on the body.
- Missed workdays: Symptoms may lead to call-outs, restricted duty, or medical appointments.
- Reduced job satisfaction: A role that once felt rewarding may become difficult to sustain.
- Burnout risk: Daily physical strain can make work feel more mentally and physically draining.
The question “Should I leave bedside nursing because of back pain?” is one of the most emotionally loaded searches a nurse can make. We address it directly at the end of this article, because you deserve a real answer, not just platitudes.
How to Prevent Back Pain as a Healthcare Worker: Practical Strategies
Back pain prevention for nurses is not about working more carefully. It is about changing the systems and habits that put your spine at risk in the first place.
Use Mechanical Lift Equipment Every Time
Safe patient handling programs help reduce the risk of injury from manual lifting. When equipment such as a Hoyer lift, ceiling lift, or sit-to-stand lift is available, it should be used instead of a manual transfer. A few extra minutes with the right device can help prevent avoidable strain.
Gait belts and transfer belts should be non-negotiable for any assisted ambulation or pivot transfer. A slide board can help reduce lower-back strain during lateral transfers compared with manually pulling a patient.
Ergonomic Practices to Build Into Every Shift
- Set the bed height to your waist level before every patient interaction. Most nurses skip this step and pay for it over time.
- Face the direction of movement. Never twist your lumbar spine while holding weight.
- Keep patients close to your body during transfers. Distance multiplies the force on your spine exponentially.
- Ask for help. A two-person transfer is not a sign of weakness. It is standard of care.
- Take micro-breaks when possible. Even 60 seconds of spinal decompression (standing upright, hands on lower back, gentle extension) can reduce cumulative load.
Ergonomic Equipment Worth Knowing
- Back brace for nurses: Lumbar support braces may provide temporary support during demanding shifts, but they should not be used as a substitute for proper body mechanics or safe lifting practices.
- Compression socks and anti-fatigue mats: They may reduce lower-extremity fatigue and support better posture as the shift progresses.
- Ergonomic nursing shoes: Proper arch support reduces the chain reaction from foot fatigue to lumbar strain.
Workers should follow workplace policy when choosing support devices for specific tasks.
Proper Body Mechanics for Patient Transfers: Step-by-Step Guide
Mastering body mechanics for nurses is the single most protective habit you can build. These steps apply to most assisted transfers:
Bed-to-Chair Transfer with Gait Belt (Two-Staff Assist)
- Explain the procedure to the patient and get their cooperation.
- Raise the bed to a height level with your hip joints.
- Apply the gait belt snugly around the patient’s waist, over clothing.
- Position the chair at a 45-degree angle to the bed on the patient’s stronger side.
- Each staff member should stand on one side of the patient with feet shoulder-width apart and knees slightly bent.
- On a coordinated count, assist the patient to a standing position using the gait belt handles. Do not grab clothing or underarms.
- Pivot with your feet. Do not twist your spine. Move your feet toward the chair.
- Lower the patient slowly, bending at the hips and knees. Keep the load close to your body.
- Confirm patient comfort and remove the gait belt.
If a patient cannot bear weight, staff should use a full-body lift, such as a Hoyer lift or ceiling lift, instead of a manual transfer. Using a gait belt with a non-weight-bearing patient is a safety violation, not a practical shortcut.
The Best Exercises and Stretches for Nurses with Back Pain
Exercises for nurses with back pain should accomplish two things: strengthen the muscles that protect your spine and decompress the structures that get loaded during shifts. Here is a practical routine you can complete in under ten minutes.
End-of-Shift Decompression Routine (5 to 7 Minutes)
1. Child’s Pose (Lumbar Decompression)
Kneel, sit back toward your heels, and extend arms forward on the floor. Hold for 45 to 60 seconds. This decompresses the lower lumbar spine, including the L4-L5 and L5-S1 areas.
2. Cat-Cow Stretch (Spinal Mobility)
On hands and knees, alternate between arching your back upward (cat) and dropping your belly toward the floor (cow). 10 repetitions. Restores the range of motion lost during prolonged static postures.
3. Hip Flexor Lunge Stretch (Priority for Night Shift Workers)
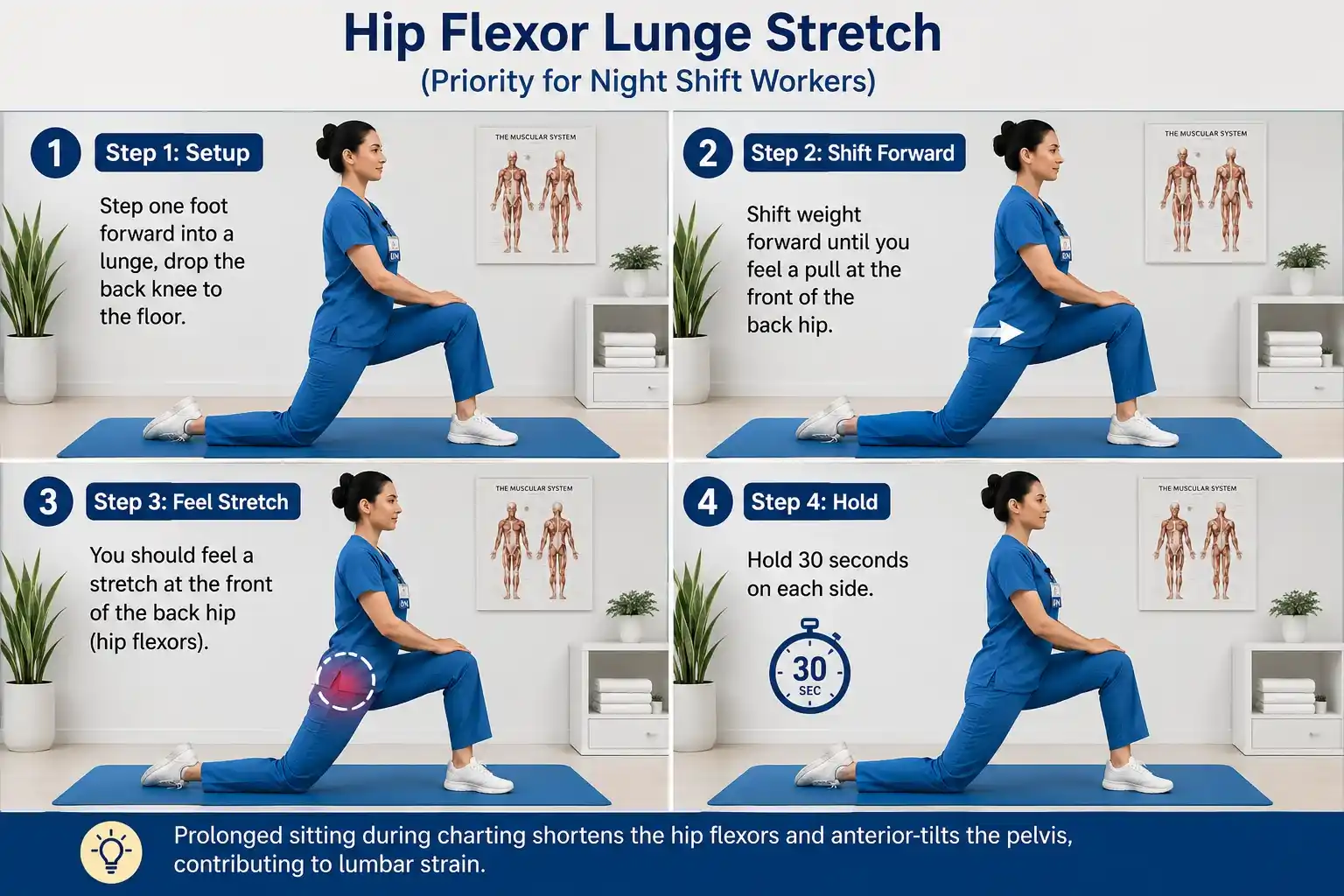
Step one foot forward into a lunge, drop the back knee to the floor, and shift weight forward until you feel a pull at the front of the back hip. Hold 30 seconds on each side. Prolonged sitting during charting shortens the hip flexors and anterior-tilts the pelvis, contributing to lumbar strain.
4. Supine Knee-to-Chest (Nerve Root Decompression)
Lie on your back and pull both knees toward your chest. Hold 30 seconds. This reduces lumbar disc pressure more than any standing position.
5. Bird Dog (Core Stability)
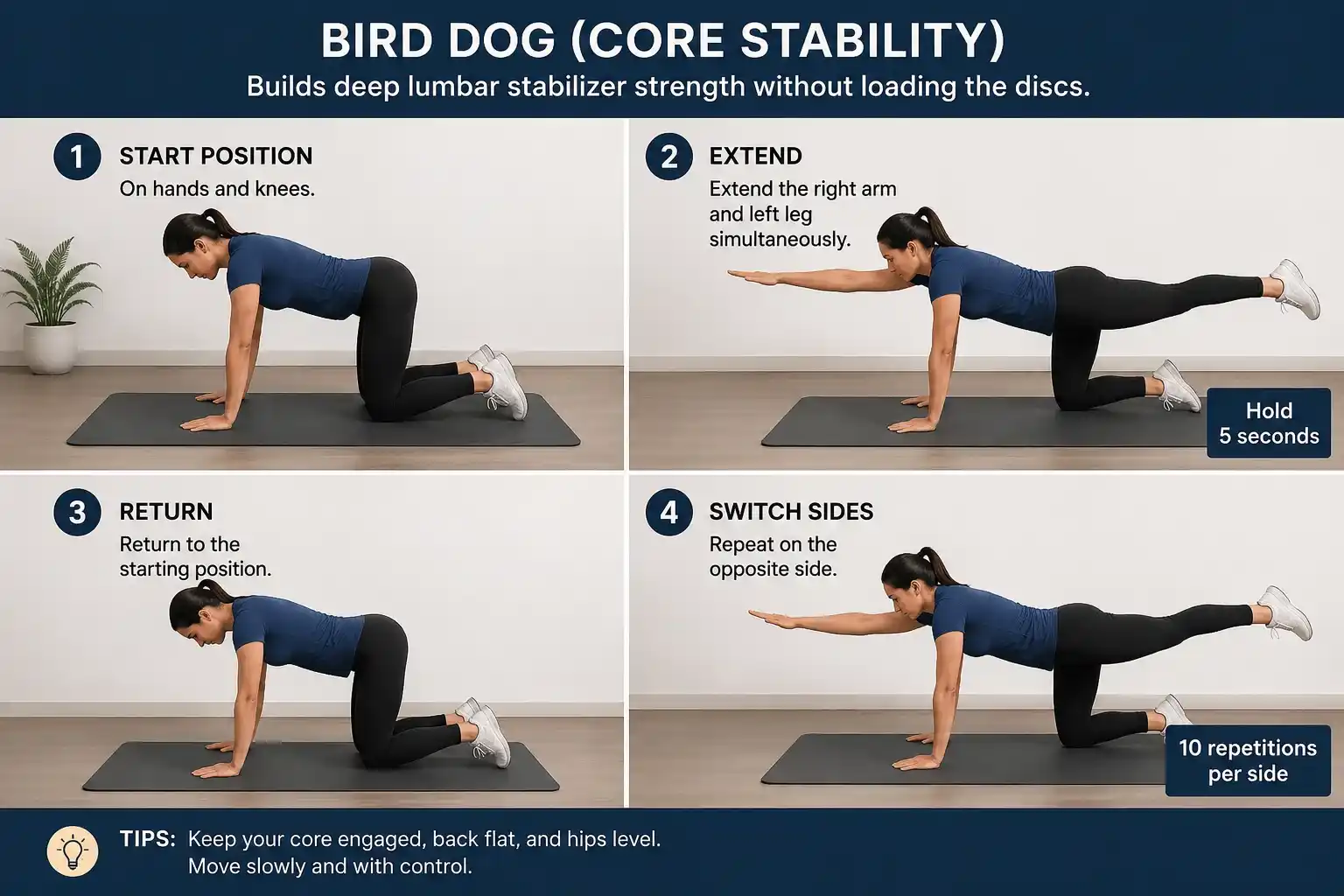
On hands and knees, extend the right arm and left leg simultaneously. Hold 5 seconds. Return and switch sides. 10 repetitions per side. This builds deep lumbar stabilizer strength without loading the discs.
6. Glute Bridge (Posterior Chain Activation)
Lie on your back, feet flat on the floor, knees bent. Press through your heels and lift your hips until your body forms a straight line from shoulders to knees. Hold 3 seconds, lower slowly. 15 repetitions. Weak glutes are one of the most underappreciated contributors to lower back pain.
On-Shift Stretches (60-Second Breaks)
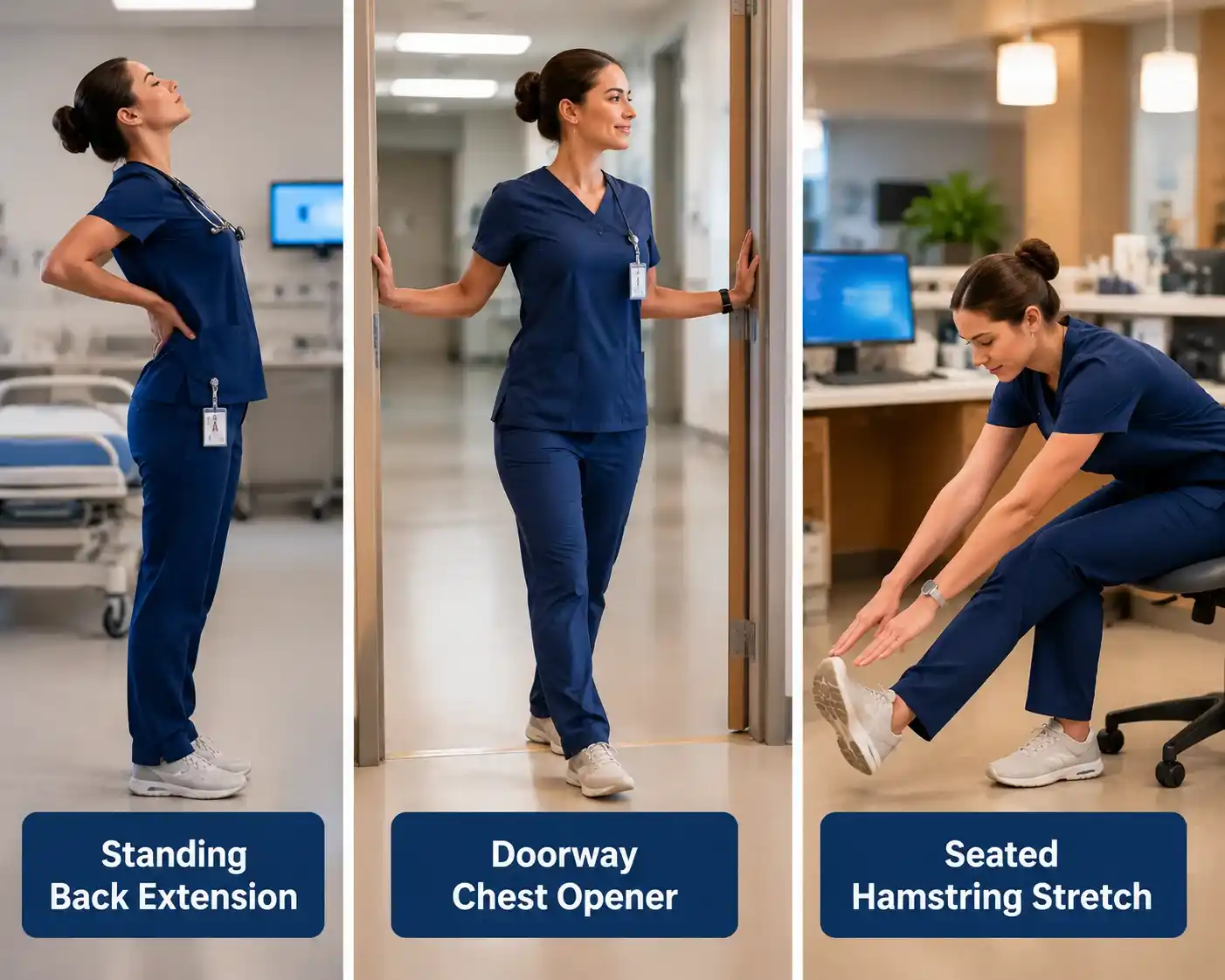
- Standing back extension: Place your hands on your lower back and gently extend backward. It may help balance the forward-bending posture often used during patient care tasks.
- Doorway chest opener: Hands on either side of a doorframe, step forward to open chest and anterior shoulder. Reverses the rounded-shoulder posture from charting.
- Seated hamstring stretch at the nurses’ station: Extend one leg straight, flex the foot, and lean forward gently. Tight hamstrings are a direct contributor to lower back strain.
When to See a Doctor: Back Pain Red Flags You Cannot Ignore
Quick Answer: According to Mayo Clinic, back pain needs emergency medical care if it causes new bowel or bladder control problems, occurs with fever, or follows trauma such as a bad fall, car crash, or sports injury.
Mayo Clinic also advises immediate medical care for severe low back pain with weakness, numbness, or tingling in one or both legs, unexplained weight loss, or pain that is constant or intense.
These symptoms may signal a serious condition, including cauda equina syndrome, infection, fracture, or nerve compression. Do not wait for a scheduled appointment if these red flags appear.
Seek urgent evaluation for:
- New bladder or bowel dysfunction following a back injury.
- Progressive leg weakness or numbness that is worsening.
- Back pain that wakes you from sleep and is not relieved by any position.
- Pain radiates into both legs simultaneously.
- Back pain following significant trauma (fall, MVA, heavy, sudden load).
Schedule a non-urgent appointment for:
- Sciatica or radiculopathy that does not improve after 2 to 4 weeks.
- Suspected disc herniation (leg pain worse than back pain, follows a dermatomal pattern).
- Pain that significantly limits your ability to perform ADLs or work tasks.
- Any recurrence of a previously diagnosed back condition.
Spinal stenosis and spondylolisthesis are also conditions that can develop or worsen with repetitive occupational loading. Do not self-diagnose or self-treat beyond standard first aid.
Workers’ Compensation and Back Pain: What Healthcare Workers Should Know
If back pain is work-related, the worker should report it through the employer’s workers’ compensation process. Rules, deadlines, approved doctors, and benefits vary by state, so workers should follow workplace policy and contact their state workers’ compensation office if needed.
To protect the record, workers should:
- Report the problem to a supervisor as soon as possible.
- Complete an incident or injury report if required.
- Seek medical evaluation through the proper workplace process.
- Keep copies of reports, medical notes, work restrictions, and messages with HR or management.
- Ask about modified duty if regular tasks are not medically safe.
- Contact the state workers’ compensation office or a qualified attorney if a claim is denied, delayed, or unclear.
You also have rights under the Americans with Disabilities Act (ADA) if your back condition qualifies as a disability. This includes the right to request reasonable accommodations such as modified duties, use of lift equipment, or scheduling adjustments.
Safe Patient Handling Programs: What Healthcare Facilities Should Provide
Safe patient handling programs are designed to reduce strain during lifting, transferring, repositioning, and moving patients. OSHA says patient transfer and lifting devices are key parts of an effective program, along with hazard assessment, equipment, care planning, staff training, and program review.
A strong, safe patient handling program may include:
- A written policy that limits manual patient lifting.
- Mechanical lift equipment, such as ceiling lifts, floor lifts, sit-to-stand lifts, and lateral transfer devices.
- Staff training on equipment use and safe transfer procedures.
- Patient assessment tools before transfers.
- Clear communication between staff before high-risk moves.
- Reporting steps for unsafe conditions or post-incident follow-up.
- Regular review of equipment access, training, and program effectiveness.
Some states have their own safe patient handling laws, but requirements vary. Facilities should follow federal safety guidance, state law, and internal workplace policy.
If workers believe patient handling conditions are unsafe, they can report the concern through workplace channels or file a safety complaint with OSHA. OSHA also allows anonymous safety complaints and separate whistleblower complaints for retaliation or threats.
Should I leave bedside nursing because of back pain?
This is not a question with a universal answer, but it deserves a real framework, not false reassurance. Leaving bedside nursing is not a failure. Nursing careers span many settings. Informatics, care coordination, education, administration, legal nurse consulting, and telehealth all value your clinical background without the physical demands of bedside care.
Consider leaving bedside nursing if:
- You have a documented structural injury (significant disc herniation, spinal stenosis, spondylolisthesis) that your spine specialist has told you will worsen with continued patient handling.
- You have already tried modified duty, and it is not sustainable in your facility.
- The pain has progressed to affecting your daily function outside of work.
- You are masking pain with medications to work, which creates both a safety risk for patients and a health risk for you.
- You are experiencing back pain and nursing burnout together, which compounds the psychological damage.
Consider continuing with modifications if:
- Your injury is acute or subacute, and you have not fully completed physical therapy.
- Your facility can realistically offer a position with limited lifting (case management, utilization review, quality, education, and telehealth nursing).
- Your pain is manageable with good body mechanics, equipment, and self-care.
- You have not yet seen a spine specialist or occupational medicine physician.
Frequently Asked Questions
1. Can wearing lead aprons in radiology or cath lab work contribute to back pain?
Yes, it can. Lead aprons add weight to the body during long procedures, which may increase strain on the back, neck, shoulders, and legs, especially when workers stand for long periods. Studies have examined lead apron use as a possible occupational risk factor for musculoskeletal discomfort among radiology and cath lab staff.
2. How does working in isolation rooms increase physical strain during patient care?
Isolation-room care may increase strain because staff often work in PPE, move carefully in limited space, and may need extra steps to enter, exit, gather supplies, and assist patients. Prolonged PPE use has also been linked with physical discomfort and workload challenges among healthcare workers.
3. Can pushing heavy medication carts or equipment carts strain the lower back?
Yes. Pushing or pulling heavy carts can place stress on the lower back, shoulders, arms, and legs, especially when carts are overloaded, hard to steer, or moved across long distances.
Bottom Line
Back pain in healthcare workers is not just a normal part of the job; it is often a sign that the body needs better support, safer movement, and timely care. By improving posture, using proper lifting techniques, asking for help when needed, and taking small recovery breaks during long shifts, healthcare staff can protect their backs and continue caring for others without ignoring their own wellbeing.
Disclaimer: This article is for educational purposes only and is not medical or legal advice. Consult a qualified professional for personal guidance.